Please Note: Pages 1-14 are for Physician Medical Licensure only. Pages are for Physician Assistants Only.
|
|
|
- Rose Weaver
- 6 years ago
- Views:
Transcription


1 Please Note: Pages 1-14 are for Physician Medical Licensure only. Pages are for Physician Assistants Only.
2 Oklahoma State Board of Medical Licensure and Supervision 101 NE 51 st St. Oklahoma City, OK Main Number: (405) Ext. 170 Fax: (405) Instructions for Applying for Physician Medical Licensure
3 Oklahoma State Board of Medical Licensure and Supervision Instructions for Applying for Licensure/Examination/Reinstatement The information contained herein is vital to the successful completion of your application and timely consideration of your request for licensure/reinstatement. Questions or challenges regarding application requirements should be addressed in writing to the Board Secretary. Lengthy telephone conversations with staff delay the overall ability to process applications. You will be notified that your application has been received by the Board Office and of all deficiencies in the application you submitted. You will also be notified how to check the status of your application on our web site: The instructions are for your benefit, designed to reduce the need for requests for information after your application has been submitted. Once your application is complete, Board action can be expected within thirty (30) days. Definitions Act means the Oklahoma Allopathic Medical and Surgical Licensure and Supervision Act, 59 O.S. Section 480 et seq. APA means either or both Article I and Article II, as applicable, of the Administrative Procedures Act, 75 O.S. 1991, Section 250 et seq., as amended. Applicant means a person who applies for licensure from the Board. Board means the Oklahoma State Board of Medical Licensure and Supervision. Foreign applicant means an applicant who is a graduate of a foreign medical school. Foreign medical school means a medical school located outside of the United States. Secretary means the Secretary of the Board. A. Options Applications for licensure may be based on: 1. Endorsement of a current license held in any other state of the United States, Territory of the United States, District of Columbia, or Canada; or 2. Examination. B. Reinstatement An applicant for reinstatement shall meet all requirements in effect at the time reinstatement is requested. Upon receipt of your application and fee, you will be notified in writing what documentation is required to complete your application. C. Temporary Licensure The Board may authorize the Secretary to issue a Temporary Medical License for the intervals between Board meetings. Such Temporary License shall be granted only when the Secretary is satisfied as to the qualifications of the applicant to be licensed under this Act but where such qualifications have not been verified to the Board. Such a license shall: 1. Be granted only to an applicant demonstrably qualified for a full and unrestricted medical license; 2. Automatically terminate on the date of the next Board meeting at which the applicant may be considered for a full and unrestricted medical license. An application for Temporary Licensure must be made by written request and include all appropriate fees. C. Fees 1. All fees are non-refundable. 2. Fees must be paid online as part of the online application process. Fees returned by the payer s financial institution must be replaced by a certified check or money order and include a $30 returned check processing fee. Oklahoma State Board of Medical Licensure and Supervision Uniform Application Instructions Revised February 2016 Page 1 of 6
4 Medical License Fee... $500 Temporary License Fee $250 First Year Post-Graduate Training License Fee.... $250 Reprocessing Fee.... $125 D. Examinations 1. Applicants who took the FLEX prior to June 1985 must have passed the examination with a FLEX weighted average of 75 or higher attained in one sitting. Scores that have been "factored" or scores from parts of the examination taken in separate sittings combined to achieve a 75 FLEX weighted average are not acceptable. Scores rounded off to achieve a 75 FLEX weighted average are not acceptable. 2. Scores achieved in the two-component FLEX examination must be 75 or higher in each component. Components may have been taken in separate jurisdictions or at separate sittings. 3. The Board will accept the following combinations of the USMLE, NBME, and FLEX examinations: a. NBME Part 1 or USMLE Step 1 plus NBME Part 2 or USMLE Step 2 plus NBME Part 3 or USMLE Step 3; b. FLEX Component 1 plus USMLE Step 3; or c. NBME Part 1 or USMLE Step 1 plus NBME Part 2 or USMLE Step 2 plus FLEX Component All steps of the licensure examination must be passed within ten (10) years. 5. If using the USMLE examination as the required licensure examination, in order to be eligible for a training license, all applicants must have passed USMLE Step 1 and Step 2. All applicants with a medical school graduation date in 2005 or later must pass USMLE Step 1 and USMLE Step 2 Clinical Skills (CS) and USMLE Step 2 Clinical Knowledge (CK). Additionally, those with a graduation date prior to 2005 who have not passed the Step 2 CK taken on or before June 30, 2005 must pass the Step 2 CS. When applying for a full, unrestricted medical license, an individual must pass Step 3 in addition to the requirements listed previously. 6. Any applicant who fails any part of a licensing examination three times is not eligible for a license. A score of incomplete is considered a failing score. If a combination of NBME, FLEX and/or USMLE is utilized, any applicant who has failed more than six (6) examinations is not eligible for a license. If an applicant has achieved certification by an American Board of Medical Specialties (ABMS) Board, the Board may grant an exception. 7. All applicants for initial licensure as a physician and surgeon in Oklahoma shall take and pass with a score of at least 75% a written examination covering medical jurisprudence. The examination shall specifically include, but not be limited to, the Oklahoma Medical Practice Act; Oklahoma Administrative Code; the prescribing, administering and dispensing of medications and controlled dangerous substances; pharmacy law; and licensure procedures. In the event of three failures, the applicant must meet with the Board Secretary in order to devise a study plan prior to taking the examination again. NOTE: We must be in receipt of your exam scores in order for the Board Secretary to consider issuing a Temporary License. E. Application Requirements 1. Each applicant shall have satisfactorily completed progressive postgraduate training approved by the Board. Graduates of medical schools in the United States shall have twelve (12) months of progressive post-graduate training. Applicants from a foreign medical school shall provide the Board with proof of successful completion of twenty-four (24) months progressive post-graduate medical training, obtained in the same medical specialty, from a program approved by: a. The American Council on Graduate Medical Education (ACGME); b. The Royal College of Physicians and Surgeons of Canada; c. The College of Family Physicians of Canada; Oklahoma State Board of Medical Licensure and Supervision Uniform Application Instructions Revised February 2016 Page 2 of 6
5 d. The Royal College of Physicians of Edinburgh; e. The Royal College of Physicians of England; f. The Royal College of Physicians and Surgeons of Glasgow; or g. The Royal College of Surgeons in Ireland. 2. Graduates of foreign medical schools must submit a tape-recorded reading of a written selection created by the Board and evaluated by the Secretary as to the ability of the applicant to communicate in the English language or take an oral examination as determined by the Board. Additional information will be sent upon receipt of application. 3. Applicants for licensure will be required to request an Extended Background Check (EBC) by completing the online EBC Authorization Form. 4. All sections of the online Uniform Application for Physician State Licensure, including forms and state addenda, must be completed to the best of your knowledge. See G. Uniform Application Core Instructions for guidance. 5. All education, training, and examination must be verified. You may use the Federation Credentials Verification Service (FCVS) for verifying your credentials, or you may verify your credentials on your own. a. FCVS requires a one-time submission of identification, education, and training documents from primary sources for verification. Once this has been done and your permanent physician Profile is established, your information is securely stored by the Federation of State Medical Boards (FSMB). Your Profile can be sent to other licensing boards and health care entities at any time in the future, provided it is up to date and each board or entity is designated to receive it. To begin your Initial (First Time) or Subsequent (Update) FCVS Application, visit fsmb.org/licensure/fcvs/ and sign in. b. If you choose to verify your credentials on your own, you must submit the following to the Board: i. Pre-Medical School. Official transcripts from all educational institutions attended (after high school) must be submitted in a sealed envelope directly from the institution. ii. Medical School. Graduation from medical school must be verified by submitting the Medical School Verification form in the Uniform Application. More information can be found in section G, number 5 of these instructions. iii. Post-Graduate Training. All completed training must be verified by submitting the Postgraduate Training Verification form in the Uniform Application. More information can be found in section G, number 5 of these instructions. Applicants for a special license to begin postgraduate training must have their prospective program complete this form to verify acceptance into the program. iv. English Proficiency Examination (Foreign Medical School Graduates). Graduates of foreign medical schools must submit a tape-recorded reading of a written selection created by the Board and evaluated by the Secretary as to the ability of the applicant to communicate in the English language or take an oral examination as determined by the Board. Examination will be sent upon receipt of application. v. Translations (Foreign Medical School Graduates). Graduates of foreign medical schools whose documents are not printed in the English language shall provide original translations. United States Consulates and formal foreign language education programs accredited by the North Central Association of Colleges and Schools are approved to provide translations to the Board. An applicant may request to use another translator. Such a request must be made in writing and include the proposed translator s name, address, and qualifications to support the approval of the request. Both the applicant and the translator shall attest to the accuracy of the translation. vi. ECFMG Verification (Foreign Medical School Graduates). Graduates of foreign medical schools must provide verification of ECFMG certification. More information can be found in section G, number 2 of these instructions. vii. Clerkships (Foreign Medical School Graduates). Effective January 1, 2004, an applicant that graduated from a foreign medical school after July 1, 2003 who completed clerkships in the United States, its territories or possessions, must have done the clerkships in hospitals or schools that have Oklahoma State Board of Medical Licensure and Supervision Uniform Application Instructions Revised February 2016 Page 3 of 6
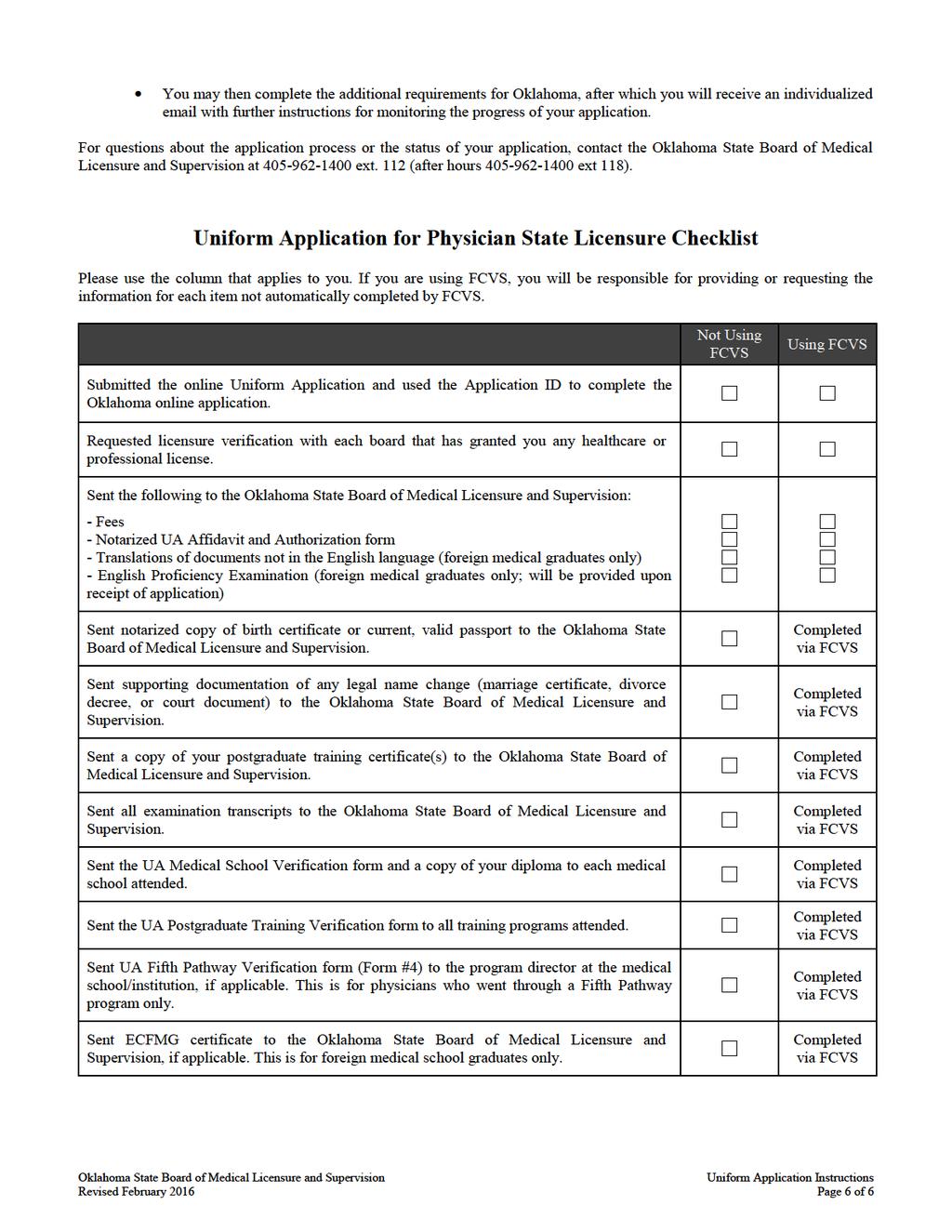
6 F. General Application Process programs accredited by the Accreditation Council for Graduate Medical Education (ACGME). A foreign medical school graduate who did clerkships in the United States must provide documentation regarding the clerkships. Every clerkship must be verified by submitted a completed Verification of Clinical Clerkship form (see addenda; signed by the program director or instructor and impressed with the institution s seal). viii. Licensing Examinations. Applicants must request that test scores be submitted to the Board directly from the Federation of State Medical Boards or the National Board of Medical Examiners, depending on the type of examination taken. More information can be found in section G, number 2 of these instructions. This office may contact other sources for verification of information contained in your application. Your application will not be considered complete until the EBC and all other requests for verification have been received. Once complete, applications are circularized to Board members for consideration. If all Board members approve the application, a license may be issued. Should one or more Board member fail to approve on circularization, the application will be reviewed during the next regularly scheduled business meeting of the Board. Applications are not denied on circularization. The applicant will be notified if the application has been held and given the opportunity to meet with the Board to discuss his/her application. Even though an application is complete and all requirements are satisfied, there is no guarantee that the Board will grant licensure. The Board may find exceptions or make discoveries that will cause them not to approve an application. In such an event, the Board will clearly state the basis upon which such exceptions have been made. The Board may, at its discretion, require further proof of clinical competency. There is no way to determine how soon you will receive notification of a Board decision after you submit an application. Even though we feel the instructions are thorough, should you have questions, you may contact the Licensing Department at (405) For questions about the Uniform Application, see G. Uniform Application Core Instructions for guidance. Please utilize the checklist provided at the end of these instructions to ensure you have submitted each required item. G. Uniform Application Core Instructions Please read the following information carefully before completing your application. You will be asked to account for all time since medical school graduation, including providing your employment history, and asked to provide any information on medical malpractice claims. We recommend having this information on hand before you begin working on your UA. The UA FAQ at fsmb.org/licensure/uniform-application/faq answers the most common UA questions. If your question or issue isn t listed, contact UA customer service at or ua@fsmb.org. Provide your username and FCVS ID number if applicable. If you receive an error, a screenshot of the error along with a description of what you were doing at the time to ua@fsmb.org. Please note the following: Provide both your current home address and current practice/training address, otherwise an error will occur. Do not enter the same address for both home and work. MD and DO licenses cannot be added or edited in the UA as all MD and DO license information comes directly into the system from the state boards. ua@fsmb.org with the correct information if changes are needed. Enter all other professional licenses (nurse, EMT, physician assistant, etc.) you have held (active or inactive) in the U.S. or Canada. Request verification from these boards as well. If you hold licenses in countries outside the U.S. or Canada, please provide that information on a separate sheet of paper to the Board. If you have military or locum tenens assignments, you must list each location/assignment separately. Oklahoma State Board of Medical Licensure and Supervision Uniform Application Instructions Revised February 2016 Page 4 of 6
7 Clinical time indicates time spent with patients. Administrative indicates time spent on paperwork. To open an already submitted UA for editing, select the Board from the State Board section. Update your UA as needed, then submit your UA to the Board. In addition to completing the core UA online, all applicants must: Submit a notarized UA Affidavit and Authorization for Release of Information form to the Board. The UA Affidavit is separate from the FCVS Affidavit and must be sent to the Board, not to FCVS or FSMB. Attach a recent (fewer than 90 days old) two inch by two inch (2 x 2 ) passport quality, color photograph of yourself in the space provided. Have each full, temporary, training, or limited healthcare or profession license or certification you have ever held in the U.S. or Canada verified by the granting board, whether active or inactive. Determine the fees and preferred verification method for each medical board using the resource at Use the UA Licensure Verification Form for boards that need a written request. If the verifying board uses VeriDoc or another method, use VeriDoc or the preferred method instead of using the UA form. If you are using FCVS for credentials verification, Do not complete the UA Medical Education Verification, Postgraduate Training Verification, or Fifth Pathway Verification forms. Do not send any identity documents, transcripts, certificates, or examination scores to the Board. FCVS handles all of this for you. If you are not using FCVS for credentials verification, Send to the Board a certified copy of a legal name change document (marriage certificate, divorce decree, court order) if your name is not the same on all of your submitted documents. Contact each appropriate examination entity to have a certified transcript of your scores sent directly from the exam entity to the Board. If you have taken any component of the NBME in conjunction with another exam (USMLE/FLEX), request your transcript of scores from the NBME. For exam entity contact information, see the UA FAQ at Complete the UA Medical Education Verification, Postgraduate Training Verification, and Fifth Pathway Verification (if applicable) forms as directed on each form. The UA Medical School Verification form should be accompanied by a copy of your diploma if you graduated from that school. A certified transcript must be sent to the Board from the appropriate educational institution. If your transcript or any other document submitted is in a language other than English, also provide a certified translation. If you are an International Medical Graduate, request from ECFMG that your ECFMG certificate, Fifth Pathway Program Certificate, and/or FMGEMS certificate be sent to the Board, as applicable. See the UA FAQ at the link above for contact information. H. State Specific Requirements In lieu of a Uniform Application addendum, you will need to visit the Board s website and complete the state specific requirements at You must create a login to the Board s online application system either before or after submitting your Uniform Application through FSMB. Once you have logged into the Board s website, you will be asked to provide a Submit ID or Application ID. Do not use your Federation ID or FCVS ID. The Application ID is found within the confirmation you receive after submitting the Uniform Application. If the Uniform Application is resubmitted, a new ID will be generated. Entering your Application ID will import your information from the UA into the Oklahoma application. Oklahoma State Board of Medical Licensure and Supervision Uniform Application Instructions Revised February 2016 Page 5 of 6
8
9 Affidavit and Authorization for Release of Information Mail this completed notarized form to: Oklahoma State Board of Medical Licensure and Supervision P.O. Box 18256; Oklahoma City, OK Applicant: Sign this form with attached photo in the presence of a notary public. Send this notarized form with any other required materials to the Board at the address listed above. If you are using FCVS for credentials verification, you must also send the separate FCVS affidavit form to FCVS if you have not already done so. I, the undersigned, being duly sworn, hereby certify under oath that I am the person named in this application, that all statements I have made or shall make with respect thereto are true, that I am the original and lawful possessor of and person named in the various forms and credentials furnished or to be furnished with respect to my application, and that all documents, forms, or copies thereof furnished or to be furnished with respect to my application are strictly true in every aspect. I acknowledge that I have read and understand the Uniform Application for Physician State Licensure and have answered all questions contained in the application truthfully and completely. I further acknowledge that failure on my part to answer questions truthfully and completely may lead to my being prosecuted under appropriate federal and state laws. I authorize and request every person, hospital, clinic, government agency (local, state, federal, or foreign), court, association, institution, or law enforcement agency having custody or control of any documents, records, and other information pertaining to me to furnish to the Board any such information, including documents, records regarding charges or complaints filed against me, formal or informal, pending or closed, or any other pertinent data, and to permit the Board or any of its agents or representatives to inspect and make copies of such documents, records, and other information in connection with this application. I hereby release, discharge, and exonerate the Board, its agents or representatives, and any person, hospital, clinic, government agency (local, state, federal, or foreign), court, association, institution, or law enforcement agency having custody or control of any documents, records, and other information pertaining to me of any and all liability of every nature and kind arising out of investigation made by the Board. I will immediately notify the Board in writing of any changes to the answers to any of the questions contained in this application if such a change occurs at any time prior to a license to practice medicine being granted to me by the Board. I understand my failure to answer questions contained in this application truthfully and completely may lead to denial, revocation, or other disciplinary sanction of my license or permit to practice medicine. Applicant Photograph Securely tape or glue a recent (less than 6 month old) front-view 2 x 2 passport-type color photo of yourself in this square. Applicant s signature (must be signed in the presence of a notary) Applicant s printed last name Applicant s printed first name, middle initial, and suffix (e.g., Jr.) Date of signature (must correspond to date of notarization) -fold up- To fit this form in a standard envelope, fold the bottom portion under the photograph toward the top, and then fold the top edge to the new bottom edge. Notary -fold up- State of, County of, I certify that on the date set forth below, the individual named above did appear personally before me and that I did identify this applicant by: (a) comparing his/her physical appearance with the photograph on the identifying document presented by the applicant and with the photograph affixed hereto, and (b) comparing the applicant s signature made in my presence on this form with the signature on his/her identifying document. The statements on this document are subscribed and sworn to before me by the applicant on this day of, 20. Notary Public Signature: My Notary Commission Expires: (NOTARY PUBLIC SEAL) Oklahoma State Board of Medical Licensure and Supervision UA Affidavit & Authorization for Release of Information February 2016 Page 1 of 1
10 Licensure Verification Form Applicant: Complete this form as directed in the left sidebar. Licensing Board: Complete this form as directed. Send the completed verification to the Oklahoma State Board of Medical Licensure and Supervision Applicant: Send this form and any applicable fee to each board you have held a full, temporary, training, or limited license with that requires a written request for license verification. To determine each board s fees and licensure verification requirements, see licensure/uniformapplication/. Section 1: Applicant Information Last name: Suffix: Degree Type: M.D. D.O. First name: Middle name: Date of Birth: Social Security Number*: *The social security number is to be used for purposes of identification only and may not be used for any other reason. Authorization: I am applying for a license to practice medicine. The Board I am applying to requires that this form be completed by each state or Canadian province in which I hold or have held licenses, whether now current or not. I authorize the licensing agency of the state/province of to provide any and all information pertaining to license number to the following Board: Board name: Oklahoma State Board of Medical Licensure and Supervision Mailing address: P.O. Box City/State/Zip: Oklahoma City, OK Applicant signature: Date: Licensing Board: Complete section 2. Send this form to the board listed in section 1. You may instead provide electronic licensure verification to the board listed in section 1. Section 2: Licensure Verification Name of Licensee: Last First Middle Suffix Issuing State Board: License number: License type: Issue date: Expiration date: Is this license current? Yes No If not current, please explain: 1. Have formal disciplinary proceedings been initiated against applicant s license by a disciplinary authority in your state? Yes No Cannot answer under state law If yes, please explain: 2. Has the applicant ever been warned, censured, placed on probation, formal consent, reprimand, or in any other manner disciplined, or has the applicant s license ever been revoked, suspended, or, in any other manner, limited by a licensing or disciplinary authority in your state? Yes No Cannot answer under state law If yes, please explain: I CERTIFY THAT to the best of my knowledge and belief, the foregoing is a true, accurate, and complete statement of the record of the individual named on this form. AFFIX BOARD SEAL HERE (If no seal is available, this form must be notarized.) Signature: Print name: Title: Date: Uniform Application for Physician State Licensure Applicant Name: Licensure Verification Form February 2016 Page 1 of 1
11 Medical School Verification Form Applicant: Complete this form as directed in the left sidebar. Medical School: Complete this form as directed. Send the completed verification to the Oklahoma State Board of Medical Licensure and Supervision. Applicant: Complete section 1. Send this form and a copy of your medical school diploma to the current Dean of your medical school. Copy this form for multiple schools. If you are using FCVS for credentials verification, do not complete this form. FCVS handles this verification for you. Section 1: Applicant Information Last name: Suffix: Degree Type: M.D. D.O. First name: Middle name: Date of Birth: Social Security Number*: Name if different when diploma awarded: Name of medical school: *The social security number is to be used for purposes of identification only and may not be used for any other reason. Waiver for Release of Information: I authorize the medical school listed above to provide any and all information pertaining to my medical education at that institution to the Board listed below. I request that the Dean or a designated official complete Section 2 of this form and seal the copy of my diploma (attached), then return this form, the sealed diploma copy, and a copy of my official transcripts to the Board listed below at the given address. Board name: Oklahoma State Board of Medical Licensure and Supervision Mailing address: P.O. Box City/State/Zip: Oklahoma City, OK Applicant signature: Date: Dean or Designated Official: Complete section 2 and certify the enclosed copy of the applicant s diploma by placing your school seal on it. Send the sealed diploma copy and an official copy of the applicant s transcripts with this completed form and any other materials to the board listed in section 1. DO NOT send this form to FCVS or FSMB. Doing so will delay the applicant s licensure process. If transcripts are not in English, an original, certified, and official English translation is required. Section 2: Medical School Verification Medical school name: School name if different when the above applicant attended: Medical school address (including city, state or province, zip code, and country as applicable): Hours of undergraduate education required for admission into your school: Total weeks of education applicant attended your school: Applicant s attendance dates: From to Graduation date: Degree: (indicate N/A if not applicable) (indicate N/A if not applicable) The questions on the following page apply to unusual circumstances that occurred during any part of the individual s medical education. Please check the appropriate response(s) and provide dates and requested information. Yes responses to any of these questions require a copy of explanatory records or a written explanation. Attach additional pages as necessary. Uniform Application for Physician State Licensure Applicant Name: Medical School Verification Form February 2016 Page 1 of 2
12 1. Do the official records for this individual reflect (an) interruption(s) or extension(s) in his/her medical education? Yes No If yes, please select the reason(s), indicate the dates of the interruption(s) or extension(s), and indicate whether the interruption(s)/ extension(s) was/were approved or unapproved. From Month/Year To Month/Year Approved Unapproved Personal/Family Academic remediation Health Financial Participation in joint degree program (e.g., MD/PhD) Participation in non-research special study (e.g., fellowship, international experience) Other: 2. Do the official records for this individual reflect that he/she was ever placed on academic or disciplinary probation during his/her medical education? Yes No If yes, please select the reason(s) for the probation, indicate the date(s) of placement on and removal from probation, and attach documentation/information of the circumstances and outcome(s). From Month/Year To Month/Year Academic probation Probation for unprofessional conduct/behavioral reasons Probation for other reason(s) (please specify): 3. Do the official records for this individual reflect that he/she was ever disciplined for unprofessional conduct/behavioral reasons by the medical school or parent university? Yes If yes, please attach documentation/information of the circumstances and outcome(s). No 4. Do the official records for this individual reflect that he/she was ever the subject of negative reports for behavioral reasons or an investigation by the medical school or parent university? Yes No If yes, please attach documentation/information of the circumstances and outcome(s). 5. Do the official records for this individual reflect that there were ever any limitations or special requirements imposed on the individual because of questions of academic incompetence, disciplinary problems, or any other reason? Yes No If yes, please attach documentation/information of the nature of the limitations or special requirements. I CERTIFY THAT to the best of my knowledge and belief, the foregoing is a true, accurate, and complete statement of the record of the individual named on this form. Signature: AFFIX INSTITUTIONAL SEAL HERE (If no seal is available, this form must be notarized.) Print name: Title: Date: Phone number: Fax number: Uniform Application for Physician State Licensure Applicant Name: Medical School Verification Form February 2016 Page 2 of 2
13 Postgraduate Training Verification Form Applicant: Complete this form as directed in the left sidebar. Training Program: Complete this form as directed. Send the completed verification to the Oklahoma State Board of Medical Licensure and Supervision. Applicant: Complete section 1. Send this form to the current Program Director of your postgraduate training program. Copy this form for multiple training programs. If you are using FCVS for credentials verification, do not complete this form. FCVS handles this verification for you. Section 1: Applicant Information Last name: Suffix: Degree Type: M.D. D.O. First name: Middle name: Date of Birth: Social Security Number*: Name if different when diploma awarded: Name of postgraduate training program: *The social security number is to be used for purposes of identification only and may not be used for any other reason. Waiver for Release of Information: I authorize the postgraduate training program listed above to provide any and all information pertaining to my medical education at that institution to the Board listed below. I request that the Program Director or a designated official complete Section 2 of this form and send it to the Board listed below at the given address. Board name: Oklahoma State Board of Medical Licensure and Supervision Mailing address: P.O. Box City/State/Zip: Oklahoma City, OK Applicant signature: Date: Dean or Designated Official: Complete section 2. Report incomplete years separately from completed years. Report each Internship, Residency, and Fellowship separately. Use one section for each specialty/subspecialty. Provide a schedule of rotations if the specialty/subspecialty is rotating/ transitional. Send this to the board listed in section 1 with any added materials, if applicable. DO NOT send this form to FCVS or FSMB. Doing so will delay the applicant s licensure process. Section 2: Postgraduate Training Verification Institution name: Institution street address: Institution city / state or province / zip code: Affiliated medical school name: Institution / school name if different when the applicant attended: 1. Postgraduate year (e.g., 1, 2, 3, etc.): Attendance dates: From to (mm/yyyy) (mm/yyyy) Internship Residency Fellowship Research Chief Residency Unspecified Other: Specialty/Subspecialty: Successfully completed*? Yes No In progress; expected completion in (mm/yyyy) *In each year of training, did the applicant demonstrate sufficient academic and clinical ability to qualify for advancement without conditional or probationary status to the next year and next progressive level of responsibility in a designated specialty program? Accredited by: ACGME AOA APPAP CFPC LCGME RCPSC RSC None of these Uniform Application for Physician State Licensure Applicant Name: Postgraduate Training Verification Form February 2016 Page 1 of 2
14 2. Postgraduate year (e.g., 1, 2, 3, etc.): Attendance dates: From to (mm/yyyy) (mm/yyyy) Internship Residency Fellowship Research Chief Residency Unspecified Other: Specialty/Subspecialty: Successfully completed*? Yes No In progress; expected completion in (mm/yyyy) *In each year of training, did the applicant demonstrate sufficient academic and clinical ability to qualify for advancement without conditional or probationary status to the next year and next progressive level of responsibility in a designated specialty program? Accredited by: ACGME AOA APPAP CFPC LCGME RCPSC RSC None of these 3. Postgraduate year (e.g., 1, 2, 3, etc.): Attendance dates: From to (mm/yyyy) (mm/yyyy) Internship Residency Fellowship Research Chief Residency Unspecified Other: Specialty/Subspecialty: Successfully completed*? Yes No In progress; expected completion in (mm/yyyy) *In each year of training, did the applicant demonstrate sufficient academic and clinical ability to qualify for advancement without conditional or probationary status to the next year and next progressive level of responsibility in a designated specialty program? Accredited by: ACGME AOA APPAP CFPC LCGME RCPSC RSC None of these Unusual Circumstances 1. Did this individual ever take a leave of absence or break from his/her training? Yes No 2. Was this individual ever placed on probation? Yes No 3. Was this individual ever disciplined or placed under investigation? Yes No 4. Were any negative reports for behavioral reasons ever filed by instructors? Yes No 5. Were any limitations or special requirements placed upon this individual Yes No because of questions of academic incompetence, disciplinary problems, or any other reason? I CERTIFY THAT to the best of my knowledge and belief, the foregoing is a true, accurate, and complete statement of the record of the individual named on this form. AFFIX INSTITUTIONAL SEAL HERE (If no seal is available, this form must be notarized.) Signature: Print name: Title: Date: Phone number: Fax number: Uniform Application for Physician State Licensure Applicant Name: Postgraduate Training Verification Form February 2016 Page 2 of 2
15 Fifth Pathway Verification Form Applicant: Complete this form as directed in the left sidebar. Program Director: Complete this form as directed. Send the completed verification to the Oklahoma State Board of Medical Licensure and Supervision. Applicant: Complete section 1. Legibly enter your name at the bottom of both pages. Send this form to your Fifth Pathway director. If you are using FCVS for credentials verification, do not complete this form. FCVS handles this verification for you. Section 1: Applicant Information Last name: Suffix: Degree Type: M.D. D.O. First name: Middle name: Date of Birth: Social Security Number*: Name if different when certificate awarded: Name of medical school: *The social security number is to be used for purposes of identification only and may not be used for any other reason. Waiver for Release of Information: I authorize the Program Director or designated official of the Fifth Pathway program to provide any and all information pertaining to my medical education at that institution to the Board listed below. I request that the Program Director or a designated official complete Section 2 of this form and send it to the Board listed below at the given address. Board name: Oklahoma State Board of Medical Licensure and Supervision Mailing address: P.O. Box City/State/Zip: Oklahoma City, OK Applicant signature: Date: Program Director or Designated Official: Complete section 2. Send this to the board in section 1 with any added documentation, if applicable. DO NOT send this form to FCVS or FSMB. Doing so will delay the applicant s licensure process. Section 2: Fifth Pathway Verification Institution name: Institution street address: Institution city / state or province / zip code: Institution / school name if different when the applicant attended: Enrollment dates: From to Completed? Yes. Certification date: No. Withdrawal date: No. Dismissal date: In progress. Expected completion date: If the applicant withdrew or was dismissed, please explain in the space below. Attach additional information if needed. Uniform Application for Physician State Licensure Applicant Name: Fifth Pathway Verification Form February 2016 Page 1 of 2
16 Type of Clinical Rotation From To Number of Weeks Credit Unusual Circumstances 1. Did this individual ever take a leave of absence or break from his/her training? Yes No 2. Was this individual ever placed on probation? Yes No 3. Was this individual ever disciplined or placed under investigation? Yes No 4. Were any negative reports for behavioral reasons ever filed by instructors? Yes No 5. Were any limitations or special requirements placed upon this individual Yes No because of questions of academic incompetence, disciplinary problems, or any other reason? Please explain any Yes response in the blank space below. Attach additional information if needed. I CERTIFY THAT to the best of my knowledge and belief, the foregoing is a true, accurate, and complete statement of the record of the individual named on this form. AFFIX INSTITUTIONAL SEAL HERE (If no seal is available, this form must be notarized.) Signature: Print name: Title: Date: Phone number: Fax number: Uniform Application for Physician State Licensure Applicant Name: Fifth Pathway Verification Form February 2016 Page 2 of 2
17 Oklahoma State Board of Medical Licensure and Supervision 101 NE 51 st St. Oklahoma City, OK Main Number: (405) Ext. 170 Fax: (405) Instructions for Applying for Physician Assistant (PA) Licensure Oklahoma State Board of Medical Licensure and Supervision Uniform Application Instructions for Physician Assistants Only August 2017 Page 1 of 5
18 A. Application for Licensure as a PA 1. A Physician Assistant (PA) may be considered for licensure if he/she meets the following qualifications: (a) Possesses good moral character, and (b) Graduated from an accredited PA program consisting of the at least one year of classroom instruction and one year of clinical experience that included a minimum of one month each in family medicine, emergency medicine and surgery, and (c) Has passed an examination for physician assistants recognized by the Board. 2. All required documents, forms and fees must accompany each application before it will be presented to the Physician Assistant tant Advisory Committee. B. Application to practice as a PA A PA may not perform any health care services until the supervising physician and PA jointly file a current application to practice and a letter authorizing practice to begin is approved. Applicants to practice received between meetings of the Committee will be reviewed by the Secretary of the Board who may grant permission by the letter to practice temporarily until the next meeting of the Committee and the Board. C. Application and forms for licensure as a PA 1. All sections of the on-line application must be completed to the best of your knowledge. 2. The photo attached to the application MUST show the notary seal impressed partially on the photograph and partially on the application to ensure that the photo on the application was the same photo notarized. Photo must be firmly affixed to the application and must not exceed the space provided, nor obscure other information on the application. 3. Any YES answers to the questions MUST be explained in a statement, signed by the applicant, and notarized. If you answered Yes too any of the questions regarding previous arrests you must additionally submit copies of all police reports/court records. If you have previously obtained an assessment and/or been treated for the use of any drugs or chemical substance (including alcohol), please submit copies of the assessment and treatment records. 4. All education and examination must be verified. Graduation from an accredited PA program may be verified on FORM #1 to which a certified copy of the diploma is attached. Applicants must also submit a transcript of grades issued by the school. The National Commission of the Certification of Physician Assistants (NCCPA) must verify successful completion of the national certifying examination for physician assistants. In lieu of contacting your school and NCCPA, you may contact the Federation Credentials Verification Service (FCVS) and obtain the appropriate application and forms for them to verify your information (FCVS, 400 Fuller Wiser Rd. Suite 300. Euless, TX Phone: ). 5. Evidence of all current or previously issued licenses or certificates or certificate to practice as a PA must be verified on form #3 by the licensing jurisdiction granting the license/certificate. D. Application and forms to practice as a PA 1. The Primary Supervising Physician and PA must jointly complete and sing form #5, Application Practice. 2. Each alternate supervising must submit form #6. Alternate supervising physician may exercise their responsibility in the absence of the primary supervising physician and may utilize the PA only in the coverage of the primary supervising physician s practice. E. General Information 1. Physician may supervise 4 PA s except: (A) The medical director of a state institution may supervise more than 4 PA s; and (B) A physician may request approval for more than 4 PA s in the clinical aspect by presentation of the application to practice to the Physician Assistant Advisory Committee in meeting. 2. Enclosed for your information are guidelines prepared by the Board of Medical Licensure and Supervision that explain more fully the Board s positon on the PA utilization. Oklahoma State Board of Medical Licensure and Supervision Uniform Application Instructions for Physician Assistants Only August 2017 Page 2 of 5
19 Additional PA Application Instructions F. Extended Background Check All applicants for licensure are required to request an Extended Background Check (EBC) by completing the online EBC Authorization Form. G. Change In Practice Locations or Supervising Physicians 1. Any change in practice locations or primary supervising must be approved by the Board upon submission of a properly completed supplication to practice for each change. 2. Material previously submitted for the original application to practice will be reviewed and those documents already on file and verified will be transferred to the request. H. Fees (All Fees Are Non-Refundable) Current 1. Initial Licensure Fee. $ (Paid on line Do not resubmit) 2. Application to Practice Fee.. $ (Included with initial licensure fee for first time applicants) 3. Renewal Fee. $ Renewal/Late Fee (between April 1 and May 31) $ I. Renewals: 1. Licenses are renewed annually by application PRIOR to March 31 st of the subsequent year beginning April 1 and the ending the last day of March. Licenses Issued BEFORE March 31 must be renewed for the next occurring renewal period most immediately subsequent to the date of issue of the license. 2. Following initial licensure, each PA must provide evidence that he or she has successfully completed 20 hours of Category 1 approved continuing medical education each year. The CME hours shall be logged and reported to the Board on an annual basis by the Oklahoma Academy of Physician Assistants, Inc. The PA shall bear the cost of this requirement. 3. Unrenowned licenses become inactive as of April 1 and if reactivated on or after April 1, a late payment fee is assessed in addition to the renewal fee. 4. If a license is not renewed by May 31, the PA will be required to submit a new application for licensure and a new application to practice, and pay the initial licensure fees. PRACTICE MAY NOT BEGIN UNTIL APPROVED BY THE STATE BOARD OF MEDICAL LICENSURE AND SUPERVISION. TO FACILITATE THE APPLICATION AND RENEWAL PROCESS, KEEP THIS OFFICE INFORMED OF YOUR CURRENT ADDRESS AT ALL TIMES. I, the undersigned, have read the instructions and understand their content. I swear/affirm the contents of my application are true. All information supplied by application may be verified by the Oklahoma State Medical Licensure and Supervision. I have read and understand the Physician Assistant Act that I received with my application. Printed Name Date Signature Oklahoma State Board of Medical Licensure and Supervision Uniform Application Instructions for Physician Assistants Only August 2017 Page 3 of 5
20
21
University of Massachusetts Amherst
 University of Massachusetts Amherst Graduate School PLEASE READ BEFORE FILLING OUT THE RESIDENCY RECLASSIFICATION APPEAL FORM The residency reclassification officers responsible for determining Massachusetts
University of Massachusetts Amherst Graduate School PLEASE READ BEFORE FILLING OUT THE RESIDENCY RECLASSIFICATION APPEAL FORM The residency reclassification officers responsible for determining Massachusetts
WASHINGTON STATE. held other states certificates) 4020B Character and Fitness Supplement (4 pages)
 4020B Character and Fitness Supplement (4 pages)") WASHINGTON STATE TEACHER RENEWAL AND CONTINUING CERTIFICATION WAC 181-79A-250 APPLICATION INSTRUCTIONS (For more information visit our certification website at http://www.k12.wa.us/certification/) Attention:
WASHINGTON STATE TEACHER RENEWAL AND CONTINUING CERTIFICATION WAC 181-79A-250 APPLICATION INSTRUCTIONS (For more information visit our certification website at http://www.k12.wa.us/certification/) Attention:
ALL DOCUMENTS MUST BE MAILED/SUBMITTED TOGETHER
 LOUISIANA BOARD OF EXAMINERS FOR SPEECH-LANGUAGE PATHOLOGY AND AUDIOLOGY 37283 SWAMP ROAD, SUITE 3B PRAIRIEVILLE, LOUISIANA 70769 PHONE: (225) 313-6358 or (800) 246-6050 WWW.LBESPA.ORG licensure renewal
LOUISIANA BOARD OF EXAMINERS FOR SPEECH-LANGUAGE PATHOLOGY AND AUDIOLOGY 37283 SWAMP ROAD, SUITE 3B PRAIRIEVILLE, LOUISIANA 70769 PHONE: (225) 313-6358 or (800) 246-6050 WWW.LBESPA.ORG licensure renewal
THE BROOKDALE HOSPITAL MEDICAL CENTER ONE BROOKDALE PLAZA BROOKLYN, NEW YORK 11212
 THE BROOKDALE HOSPITAL MEDICAL CENTER ONE BROOKDALE PLAZA BROOKLYN, NEW YORK 11212 AGREEMENT made this day of, 200, between BROOKDALE HOSPITAL MEDICAL CENTER, a not-for-profit Hospital corporation, hereinafter
THE BROOKDALE HOSPITAL MEDICAL CENTER ONE BROOKDALE PLAZA BROOKLYN, NEW YORK 11212 AGREEMENT made this day of, 200, between BROOKDALE HOSPITAL MEDICAL CENTER, a not-for-profit Hospital corporation, hereinafter
IN-STATE TUITION PETITION INSTRUCTIONS AND DEADLINES Western State Colorado University
 IN-STATE TUITION PETITION INSTRUCTIONS AND DEADLINES Western State Colorado University Petitions will be accepted beginning 60 days before the semester starts for each academic semester. Petitions will
IN-STATE TUITION PETITION INSTRUCTIONS AND DEADLINES Western State Colorado University Petitions will be accepted beginning 60 days before the semester starts for each academic semester. Petitions will
Northwest Georgia RESA
 Northwest Georgia RESA Office of Executive Director 3167 Cedartown Hwy SE Rome, GA 30161 (706) 295-6189 Fax: (706) 295-6098 Date of Application: Date Available for Employment: Personal Information Full
Northwest Georgia RESA Office of Executive Director 3167 Cedartown Hwy SE Rome, GA 30161 (706) 295-6189 Fax: (706) 295-6098 Date of Application: Date Available for Employment: Personal Information Full
Duke University. Trinity College of Arts & Sciences/ Pratt School of Engineering Application for Readmission to Duke
 Office Use Only Durham, North Carolina Application Fee $30 received Trinity College of Arts & Sciences/ Pratt School of Engineering Application for Readmission to Duke BEFORE completing this application,
Office Use Only Durham, North Carolina Application Fee $30 received Trinity College of Arts & Sciences/ Pratt School of Engineering Application for Readmission to Duke BEFORE completing this application,
Rules of Procedure for Approval of Law Schools
 Rules of Procedure for Approval of Law Schools Table of Contents I. Scope and Authority...49 Rule 1: Scope and Purpose... 49 Rule 2: Council Responsibility and Authority with Regard to Accreditation Status...
Rules of Procedure for Approval of Law Schools Table of Contents I. Scope and Authority...49 Rule 1: Scope and Purpose... 49 Rule 2: Council Responsibility and Authority with Regard to Accreditation Status...
Thomas Jefferson University Hospital. Institutional Policies and Procedures For Graduate Medical Education Programs
 Thomas Jefferson University Hospital Institutional Policies and Procedures For Graduate Medical Education Programs Table of Contents Dispute Resolution Procedure 1 Duty Hours 2 Duty Hours Requests for
Thomas Jefferson University Hospital Institutional Policies and Procedures For Graduate Medical Education Programs Table of Contents Dispute Resolution Procedure 1 Duty Hours 2 Duty Hours Requests for
International Undergraduate Application for Admission
 CHECKLIST Application fee: US$30 (required) Completed application form Request academic records International Undergraduate Application for Admission Request exam score reports Copy of passport Completed
CHECKLIST Application fee: US$30 (required) Completed application form Request academic records International Undergraduate Application for Admission Request exam score reports Copy of passport Completed
MANDATORY CONTINUING LEGAL EDUCATION REGULATIONS PURPOSE
 MANDATORY CONTINUING LEGAL EDUCATION REGULATIONS PURPOSE The Virginia Supreme Court has established, by Rule of Court, a mandatory continuing legal education program in the Commonwealth of Virginia, which
MANDATORY CONTINUING LEGAL EDUCATION REGULATIONS PURPOSE The Virginia Supreme Court has established, by Rule of Court, a mandatory continuing legal education program in the Commonwealth of Virginia, which
Guidelines for Completion of an Application for Temporary Licence under Section 24 of the Architects Act R.S.O. 1990
 Guidelines for Completion of an Application for Temporary Licence under Section 24 of the Architects Act R.S.O. 1990 OAA-12-16 1 INDEX Page Number General... 3 Fees for Temporary Licence... 4 Appendix
Guidelines for Completion of an Application for Temporary Licence under Section 24 of the Architects Act R.S.O. 1990 OAA-12-16 1 INDEX Page Number General... 3 Fees for Temporary Licence... 4 Appendix
Verification Program Health Authority Abu Dhabi
 ONLY COMPLETE FORMS WILL BE ACCEPTED Verification Program Health Authority Abu Dhabi Facility Name (If applicable) PearsonVue Registration ID (if applicable) Personal Details: Please give your name in
ONLY COMPLETE FORMS WILL BE ACCEPTED Verification Program Health Authority Abu Dhabi Facility Name (If applicable) PearsonVue Registration ID (if applicable) Personal Details: Please give your name in
REGULATION RESPECTING THE TERMS AND CONDITIONS FOR THE ISSUANCE OF THE PERMIT AND SPECIALIST'S CERTIFICATES BY THE COLLÈGE DES MÉDECINS DU QUÉBEC
 (This version is offered as a courtesy and holds no official value.) Professional Code (R.S.Q., c. C-26, s. 93, sub. c and c.1, 94 par. i and 94.1) DIVISION I GENERAL PROVISIONS 1. The purpose of this
(This version is offered as a courtesy and holds no official value.) Professional Code (R.S.Q., c. C-26, s. 93, sub. c and c.1, 94 par. i and 94.1) DIVISION I GENERAL PROVISIONS 1. The purpose of this
ESIC Advt. No. 06/2017, dated WALK IN INTERVIEW ON
 EMPLOYEES STATE INSURANCE CORPORATION ESIC-PGIMSR & ESIC MEDICAL COLLEGE ESIC Hospital & ODC (EZ) Diamond Harbour Road, P.O. Joka, Kolkata - 700104 Tel No: (033) 24381382, Tel/Fax No: (033) 24381176 E-mail:
EMPLOYEES STATE INSURANCE CORPORATION ESIC-PGIMSR & ESIC MEDICAL COLLEGE ESIC Hospital & ODC (EZ) Diamond Harbour Road, P.O. Joka, Kolkata - 700104 Tel No: (033) 24381382, Tel/Fax No: (033) 24381176 E-mail:
Scholarship Application For current University, Community College or Transfer Students
 (AN INSTRUMENTALITY OF THE TOWN OF WESTLAKE) 2014-2015 Scholarship Application For current University, Community College or Transfer Students In 2013 TSHA awarded in excess of $420,000 (market value) scholarships
(AN INSTRUMENTALITY OF THE TOWN OF WESTLAKE) 2014-2015 Scholarship Application For current University, Community College or Transfer Students In 2013 TSHA awarded in excess of $420,000 (market value) scholarships
INTERNAL MEDICINE IN-TRAINING EXAMINATION (IM-ITE SM )
") INTERNAL MEDICINE IN-TRAINING EXAMINATION (IM-ITE SM ) GENERAL INFORMATION The Internal Medicine In-Training Examination, produced by the American College of Physicians and co-sponsored by the Alliance
INTERNAL MEDICINE IN-TRAINING EXAMINATION (IM-ITE SM ) GENERAL INFORMATION The Internal Medicine In-Training Examination, produced by the American College of Physicians and co-sponsored by the Alliance
ADULT VOCATIONAL TRAINING (AVT) APPLICATION
 APPLICATION") Attention Education Department AVT 2468 West 11 th Eugene, OR 97402 ADULT VOCATIONAL TRAINING (AVT) APPLICATION The following documents or information will be required to complete the application: Documents
Attention Education Department AVT 2468 West 11 th Eugene, OR 97402 ADULT VOCATIONAL TRAINING (AVT) APPLICATION The following documents or information will be required to complete the application: Documents
IUPUI Office of Student Conduct Disciplinary Procedures for Alleged Violations of Personal Misconduct
 IUPUI Office of Student Conduct Disciplinary Procedures for Alleged Violations of Personal Misconduct Preamble IUPUI disciplinary procedures determine responsibility and appropriate consequences for violations
IUPUI Office of Student Conduct Disciplinary Procedures for Alleged Violations of Personal Misconduct Preamble IUPUI disciplinary procedures determine responsibility and appropriate consequences for violations
American College of Emergency Physicians National Emergency Medicine Medical Student Award Nomination Form. Due Date: February 14, 2012
 Nomination Form Due Date: February 14, 2012 Please follow instructions closely, and make sure you have included all requested information listed on the checklist. Electronic submissions only. Please refrain
Nomination Form Due Date: February 14, 2012 Please follow instructions closely, and make sure you have included all requested information listed on the checklist. Electronic submissions only. Please refrain
Pierce County Schools. Pierce Truancy Reduction Protocol. Dr. Joy B. Williams Superintendent
 Pierce County Schools Pierce Truancy Reduction Protocol 2005 2006 Dr. Joy B. Williams Superintendent Mark Dixon Melvin Johnson Pat Park Ken Jorishie Russell Bell 1 Pierce County Truancy Reduction Protocol
Pierce County Schools Pierce Truancy Reduction Protocol 2005 2006 Dr. Joy B. Williams Superintendent Mark Dixon Melvin Johnson Pat Park Ken Jorishie Russell Bell 1 Pierce County Truancy Reduction Protocol
Purchase College STATE UNIVERSITY OF NEW YORK
 IMPORTANT: Your application was selected for review in a process called "Verification". We will be comparing information from your FAFSA with the documentation we have requested. If there are differences,
IMPORTANT: Your application was selected for review in a process called "Verification". We will be comparing information from your FAFSA with the documentation we have requested. If there are differences,
INDEPENDENT STUDY PROGRAM
 INSTRUCTION BOARD POLICY BP6158 INDEPENDENT STUDY PROGRAM The Governing Board authorizes independent study as a voluntary alternative instructional setting by which students may reach curricular objectives
INSTRUCTION BOARD POLICY BP6158 INDEPENDENT STUDY PROGRAM The Governing Board authorizes independent study as a voluntary alternative instructional setting by which students may reach curricular objectives
Basic Standards for Residency Training in Internal Medicine. American Osteopathic Association and American College of Osteopathic Internists
 Basic Standards for Residency Training in Internal Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 TABLE OF CONTENTS I. Introduction... 3 II Mission...
Basic Standards for Residency Training in Internal Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 TABLE OF CONTENTS I. Introduction... 3 II Mission...
Tamwood Language Centre Policies Revision 12 November 2015
 Do More, Learn More, BE MORE! By teaching, coaching and encouraging our students, Tamwood Language Centres helps students to develop their talents, achieve their educational goals and realize their potential.
Do More, Learn More, BE MORE! By teaching, coaching and encouraging our students, Tamwood Language Centres helps students to develop their talents, achieve their educational goals and realize their potential.
2012 Summer Fellowship in Translational Research & Bioethics International Institute of Bioethics & Patient Care Advancement
 2012 Summer Fellowship in Translational Research & Bioethics Dominique Monlezun, Admissions Committee Coordinator #420 Deming Pavillion~204 S. Saratoga St~ New Orleans, LA 70112 E-Mail dmonlezu@tulane.edu
2012 Summer Fellowship in Translational Research & Bioethics Dominique Monlezun, Admissions Committee Coordinator #420 Deming Pavillion~204 S. Saratoga St~ New Orleans, LA 70112 E-Mail dmonlezu@tulane.edu
Emergency Medical Technician Course Application
 Community Health Network Emergency Medical Technician Course Application January 2018 First day of Class January 8,2018 EMERGENCY MEDICAL SERVICES & EDUCATION Thank you for your consideration in choosing
Community Health Network Emergency Medical Technician Course Application January 2018 First day of Class January 8,2018 EMERGENCY MEDICAL SERVICES & EDUCATION Thank you for your consideration in choosing
APPLICATION DEADLINE: 5:00 PM, December 25, 2013
 FCAST EXCHANGE APPLICATION APPLICATION INSTRUCTIONS GLOBAL UNDERGRADUATE EXCHANGE PROGRAM IN SERBIA 2014-2015 THE GLOBAL UGRAD PROGRAM IS SPONSORED BY THE U.S. DEPARTMENT OF STATE S BUREAU OF EDUCATIONAL
FCAST EXCHANGE APPLICATION APPLICATION INSTRUCTIONS GLOBAL UNDERGRADUATE EXCHANGE PROGRAM IN SERBIA 2014-2015 THE GLOBAL UGRAD PROGRAM IS SPONSORED BY THE U.S. DEPARTMENT OF STATE S BUREAU OF EDUCATIONAL
Pharmacy Technician Program
 Pharmacy Technician Program 12800 Abrams Road Dallas, Texas 75243-2199 972.238.6950 www.richlandcollege.edu/hp Health Professions Division Pharmacy Technician Program Application Packet Equal Opportunity
Pharmacy Technician Program 12800 Abrams Road Dallas, Texas 75243-2199 972.238.6950 www.richlandcollege.edu/hp Health Professions Division Pharmacy Technician Program Application Packet Equal Opportunity
ADULT VOCATIONAL TRAINING PROGRAM APPLICATION
 Ph: ADULT VOCATIONAL TRAINING PROGRAM APPLICATION Applicant: Enclosed is the application packet you requested for the Adult Vocational Training Program (AVT). If you are a first time applicant, the AVT
Ph: ADULT VOCATIONAL TRAINING PROGRAM APPLICATION Applicant: Enclosed is the application packet you requested for the Adult Vocational Training Program (AVT). If you are a first time applicant, the AVT
Please fill in the application form below if you wish to apply for any of the study programs of the Faculty of Humanities.
 20170112-001 Application Form for International Students EÖTVÖS LORÁND UNIVERSITY FACULTY OF HUMANITIES APPLICATION FORM FOR INTERNATIONAL STUDENTS ACADEMIC YEAR 2017/2018 INTERNATIONAL STUDENT APPLICATION
20170112-001 Application Form for International Students EÖTVÖS LORÁND UNIVERSITY FACULTY OF HUMANITIES APPLICATION FORM FOR INTERNATIONAL STUDENTS ACADEMIC YEAR 2017/2018 INTERNATIONAL STUDENT APPLICATION
Santa Fe Community College Teacher Academy Student Guide 1
 Santa Fe Community College Teacher Academy Student Guide Student Guide 1 We believe that ALL students can succeed and it is the role of the teacher to nurture, inspire, and motivate ALL students to succeed.
Santa Fe Community College Teacher Academy Student Guide Student Guide 1 We believe that ALL students can succeed and it is the role of the teacher to nurture, inspire, and motivate ALL students to succeed.
Master of Philosophy. 1 Rules. 2 Guidelines. 3 Definitions. 4 Academic standing
 1 Rules 1.1 There shall be a degree which may be awarded an overall grade. The award of the grade shall be made for meritorious performance in the program, with greatest weight given to completion of the
1 Rules 1.1 There shall be a degree which may be awarded an overall grade. The award of the grade shall be made for meritorious performance in the program, with greatest weight given to completion of the
TITLE 23: EDUCATION AND CULTURAL RESOURCES SUBTITLE A: EDUCATION CHAPTER I: STATE BOARD OF EDUCATION SUBCHAPTER b: PERSONNEL PART 25 CERTIFICATION
 ISBE 23 ILLINOIS ADMINISTRATIVE CODE 25 TITLE 23: EDUCATION AND CULTURAL RESOURCES : EDUCATION CHAPTER I: STATE BOARD OF EDUCATION : PERSONNEL Section 25.10 Accredited Institution PART 25 CERTIFICATION
ISBE 23 ILLINOIS ADMINISTRATIVE CODE 25 TITLE 23: EDUCATION AND CULTURAL RESOURCES : EDUCATION CHAPTER I: STATE BOARD OF EDUCATION : PERSONNEL Section 25.10 Accredited Institution PART 25 CERTIFICATION
AFFILIATION AGREEMENT
 AFFILIATION AGREEMENT THIS AFFILIATION AGREEMENT ( Agreement ) is made and entered into as of November 14, 2011 ( Effective Date ), by and between, on behalf of its School of Public Health and Information
AFFILIATION AGREEMENT THIS AFFILIATION AGREEMENT ( Agreement ) is made and entered into as of November 14, 2011 ( Effective Date ), by and between, on behalf of its School of Public Health and Information
ARKANSAS TECH UNIVERSITY
 ARKANSAS TECH UNIVERSITY Procurement and Risk Management Services Young Building 203 West O Street Russellville, AR 72801 REQUEST FOR PROPOSAL Search Firms RFP#16-017 Due February 26, 2016 2:00 p.m. Issuing
ARKANSAS TECH UNIVERSITY Procurement and Risk Management Services Young Building 203 West O Street Russellville, AR 72801 REQUEST FOR PROPOSAL Search Firms RFP#16-017 Due February 26, 2016 2:00 p.m. Issuing
2018 Summer Application to Study Abroad
 Page 1 of 7 Attach one COLOR driver's license or passport sized photograph here. 2018 Summer Application to Study Abroad More than one photograph may be required during the application process. Check individual
Page 1 of 7 Attach one COLOR driver's license or passport sized photograph here. 2018 Summer Application to Study Abroad More than one photograph may be required during the application process. Check individual
Academic Advising Manual
 Academic Advising Manual Revised 17 July 2013 1 Academic Advising Manual Table of Contents I. Academic Advising Mission Statement. 3 II. Goals and Responsibilities of Advisors and Students 3-5 III. Characteristics
Academic Advising Manual Revised 17 July 2013 1 Academic Advising Manual Table of Contents I. Academic Advising Mission Statement. 3 II. Goals and Responsibilities of Advisors and Students 3-5 III. Characteristics
Department of Social Work Master of Social Work Program
 Dear Interested Applicant, Thank you for your interest in the California State University, Dominguez Hills Master of Social Work (MSW) Program. On behalf of the faculty I want you to know that we are very
Dear Interested Applicant, Thank you for your interest in the California State University, Dominguez Hills Master of Social Work (MSW) Program. On behalf of the faculty I want you to know that we are very
Student Policy Handbook
 Student Policy Handbook Revised September 2017 excelsior.edu LIMITATIONS Information in this Student Policy Handbook is current as of September 2017, and is subject to change without advance notice. CHANGES
Student Policy Handbook Revised September 2017 excelsior.edu LIMITATIONS Information in this Student Policy Handbook is current as of September 2017, and is subject to change without advance notice. CHANGES
Department of Education School of Education & Human Services Master of Education Policy Manual
 Department of Education School of Education & Human Services Master of Education Policy Manual Prepared by: Dr. Stacey Brown-Hobbs Elizabeth C. Monahan, PDS Liaison Edited by: Carolyn L. Cook, Director
Department of Education School of Education & Human Services Master of Education Policy Manual Prepared by: Dr. Stacey Brown-Hobbs Elizabeth C. Monahan, PDS Liaison Edited by: Carolyn L. Cook, Director
Bihar State Milk Co-operative Federation Ltd. - COMFED: P&A: Advertisement No. - 2/2014 Managing Director
 Bihar State Milk Co-operative Federation Ltd. Dairy Development Complex; Post :- B.V. College, Patna - 800014 Phone No. - 0612-2228953, 2220387, 2224083; Fax 0612-2228306 Web :- www.sudha.coop; Email:-
Bihar State Milk Co-operative Federation Ltd. Dairy Development Complex; Post :- B.V. College, Patna - 800014 Phone No. - 0612-2228953, 2220387, 2224083; Fax 0612-2228306 Web :- www.sudha.coop; Email:-
DEPARTMENT OF KINESIOLOGY AND SPORT MANAGEMENT
 DEPARTMENT OF KINESIOLOGY AND SPORT MANAGEMENT Undergraduate Sport Management Internship Guide SPMT 4076 (Version 2017.1) Box 43011 Lubbock, TX 79409-3011 Phone: (806) 834-2905 Email: Diane.nichols@ttu.edu
DEPARTMENT OF KINESIOLOGY AND SPORT MANAGEMENT Undergraduate Sport Management Internship Guide SPMT 4076 (Version 2017.1) Box 43011 Lubbock, TX 79409-3011 Phone: (806) 834-2905 Email: Diane.nichols@ttu.edu
NATIVE VILLAGE OF BARROW WORKFORCE DEVLEOPMENT DEPARTMENT HIGHER EDUCATION AND ADULT VOCATIONAL TRAINING FINANCIAL ASSISTANCE APPLICATION
 NATIVE VILLAGE OF BARROW WORKFORCE DEVLEOPMENT DEPARTMENT HIGHER EDUCATION AND ADULT VOCATIONAL TRAINING FINANCIAL ASSISTANCE APPLICATION To better assist our Clients, here is a check off list of the following
NATIVE VILLAGE OF BARROW WORKFORCE DEVLEOPMENT DEPARTMENT HIGHER EDUCATION AND ADULT VOCATIONAL TRAINING FINANCIAL ASSISTANCE APPLICATION To better assist our Clients, here is a check off list of the following
CHAPTER 30 - NC BOARD OF MASSAGE AND BODYWORK THERAPY SECTION ORGANIZATION AND GENERAL PROVISIONS
 CHAPTER 30 - NC BOARD OF MASSAGE AND BODYWORK THERAPY SECTION.0100 - ORGANIZATION AND GENERAL PROVISIONS 21 NCAC 30.0101 PURPOSE The purpose of the rules in this Chapter is to implement the provisions
CHAPTER 30 - NC BOARD OF MASSAGE AND BODYWORK THERAPY SECTION.0100 - ORGANIZATION AND GENERAL PROVISIONS 21 NCAC 30.0101 PURPOSE The purpose of the rules in this Chapter is to implement the provisions
ATHLETIC TRAINING SERVICES AGREEMENT
 ATHLETIC TRAINING SERVICES AGREEMENT THIS ATHLETIC TRAINING SERVICES AGREEMENT is made on this 17th day of May, 2017, by and between Strong Memorial Hospital/UR Medicine Sports Medicine, a division of
ATHLETIC TRAINING SERVICES AGREEMENT THIS ATHLETIC TRAINING SERVICES AGREEMENT is made on this 17th day of May, 2017, by and between Strong Memorial Hospital/UR Medicine Sports Medicine, a division of
GPI Partner Training Manual. Giving a student the opportunity to study in another country is the best investment you can make in their future
 2017 - Version 1.0 Giving a student the opportunity to study in another country is the best investment you can make in their future GPI Partner Training Manual Contents Welcome...........................
2017 - Version 1.0 Giving a student the opportunity to study in another country is the best investment you can make in their future GPI Partner Training Manual Contents Welcome...........................
CIN-SCHOLARSHIP APPLICATION
 CATAWBA INDIAN NATION SCHOLARSHIP COMMITTEE 2014-2015 CIN-SCHOLARSHIP APPLICATION The Catawba Indian Nation Higher Education Scholarship Committee Presents: THE CATAWBA INDIAN NATION SCHOLARSHIP PROGRAM
CATAWBA INDIAN NATION SCHOLARSHIP COMMITTEE 2014-2015 CIN-SCHOLARSHIP APPLICATION The Catawba Indian Nation Higher Education Scholarship Committee Presents: THE CATAWBA INDIAN NATION SCHOLARSHIP PROGRAM
PROGRAM REQUIREMENTS FOR CLINICAL FELLOWSHIP TRAINING IN GENERAL COSMETIC SURGERY
 PROGRAM REQUIREMENTS FOR CLINICAL FELLOWSHIP TRAINING IN GENERAL COSMETIC SURGERY Overview... 3 Background... 4 Qualifying Terms... 5 Fellowship Status... 6 PROGRAM REQUIREMENTS... 7 Institutional Commitment...
PROGRAM REQUIREMENTS FOR CLINICAL FELLOWSHIP TRAINING IN GENERAL COSMETIC SURGERY Overview... 3 Background... 4 Qualifying Terms... 5 Fellowship Status... 6 PROGRAM REQUIREMENTS... 7 Institutional Commitment...
Enrollment Forms Packet (EFP)
") Enrollment Forms Packet (EFP) Based on r student(s) grade and applicable circumstances, complete one enrollment package and review the information below to determine what should submit for each student
Enrollment Forms Packet (EFP) Based on r student(s) grade and applicable circumstances, complete one enrollment package and review the information below to determine what should submit for each student
CERTIFIED TEACHER LICENSURE PROFESSIONAL DEVELOPMENT PLAN
 CERTIFIED TEACHER LICENSURE PROFESSIONAL DEVELOPMENT PLAN 2016-2017 DODGE CITY PUBLIC SCHOOLS USD 443 DODGE CITY, KANSAS LOCAL PROFESSIONAL DEVELOPMENT GUIDE Table of Contents 1. General Information -
CERTIFIED TEACHER LICENSURE PROFESSIONAL DEVELOPMENT PLAN 2016-2017 DODGE CITY PUBLIC SCHOOLS USD 443 DODGE CITY, KANSAS LOCAL PROFESSIONAL DEVELOPMENT GUIDE Table of Contents 1. General Information -
Exclusions Policy. Policy reviewed: May 2016 Policy review date: May OAT Model Policy
 Exclusions Policy Policy reviewed: May 2016 Policy review date: May 2018 OAT Model Policy 1 Contents Action to be invoked by Senior Staff in Serious Disciplinary Matters 1. When a serious incident occurs,
Exclusions Policy Policy reviewed: May 2016 Policy review date: May 2018 OAT Model Policy 1 Contents Action to be invoked by Senior Staff in Serious Disciplinary Matters 1. When a serious incident occurs,
Instructions concerning the right to study
 INSTRUCTIONS 1(10) THE RIGHT TO STUDY Instructions concerning the right to study 1. Purpose of the instructions 2. Application procedures 3. Transfer applications 4. Compulsory annual registration 5. Maximum
INSTRUCTIONS 1(10) THE RIGHT TO STUDY Instructions concerning the right to study 1. Purpose of the instructions 2. Application procedures 3. Transfer applications 4. Compulsory annual registration 5. Maximum
Rules and Regulations of Doctoral Studies
 Annex to the SGH Senate Resolution no.590 of 22 February 2012 Rules and Regulations of Doctoral Studies at the Warsaw School of Economics Preliminary provisions 1 1. Rules and Regulations of doctoral studies
Annex to the SGH Senate Resolution no.590 of 22 February 2012 Rules and Regulations of Doctoral Studies at the Warsaw School of Economics Preliminary provisions 1 1. Rules and Regulations of doctoral studies
Hiring Procedures for Faculty. Table of Contents
 Hiring Procedures for Faculty Table of Contents SECTION I: PROCEDURES FOR NEW FULL-TIME FACULTY APPOINTMENTS... 2 A. Search Committee... 2 B. Applicant Clearinghouse Form and Applicant Data Sheet... 2
Hiring Procedures for Faculty Table of Contents SECTION I: PROCEDURES FOR NEW FULL-TIME FACULTY APPOINTMENTS... 2 A. Search Committee... 2 B. Applicant Clearinghouse Form and Applicant Data Sheet... 2
RECRUITMENT AND EXAMINATIONS
 CHAPTER V: RECRUITMENT AND EXAMINATIONS RULE 5.1 RECRUITMENT Section 5.1.1 Announcement of Examinations RULE 5.2 EXAMINATION Section 5.2.1 Determination of Examinations 5.2.2 Open Competitive Examinations
CHAPTER V: RECRUITMENT AND EXAMINATIONS RULE 5.1 RECRUITMENT Section 5.1.1 Announcement of Examinations RULE 5.2 EXAMINATION Section 5.2.1 Determination of Examinations 5.2.2 Open Competitive Examinations
The AAMC Standardized Video Interview: Essentials for the ERAS 2018 Season
 The AAMC Standardized Video Interview: Essentials for the ERAS 2018 Season The AAMC Standardized Video Interview: Essentials for the ERAS 2018 Season Association of American Medical Colleges Washington,
The AAMC Standardized Video Interview: Essentials for the ERAS 2018 Season The AAMC Standardized Video Interview: Essentials for the ERAS 2018 Season Association of American Medical Colleges Washington,
LAKEWOOD SCHOOL DISTRICT CO-CURRICULAR ACTIVITIES CODE LAKEWOOD HIGH SCHOOL OPERATIONAL PROCEDURES FOR POLICY #4247
 Page 2 of 14 LAKEWOOD SCHOOL DISTRICT CO-CURRICULAR ACTIVITIES CODE PHILOSOPHY It is the desire of the Lakewood School District that each student reach his or her academic potential. The Lakewood School
Page 2 of 14 LAKEWOOD SCHOOL DISTRICT CO-CURRICULAR ACTIVITIES CODE PHILOSOPHY It is the desire of the Lakewood School District that each student reach his or her academic potential. The Lakewood School
Adult Vocational Training Tribal College Fund Gaming
 Statement of Goals and Objectives Adult Vocational Training Tribal College Fund Gaming The Kaibab Band of Paiute Indians has instituted a long range goal of economic self-sufficiency and social development
Statement of Goals and Objectives Adult Vocational Training Tribal College Fund Gaming The Kaibab Band of Paiute Indians has instituted a long range goal of economic self-sufficiency and social development
Policy JECAA STUDENT RESIDENCY Proof of Legal Custody and Residency Establishment of Residency
 Policy JECAA STUDENT RESIDENCY In order to attend the Illinois Mathematics and Science Academy each year, a student must be a legal resident of the State of Illinois. In determining residency, the residence
Policy JECAA STUDENT RESIDENCY In order to attend the Illinois Mathematics and Science Academy each year, a student must be a legal resident of the State of Illinois. In determining residency, the residence
Schenectady County Is An Equal Opportunity Employer. Open Competitive Examination
 Schenectady County Is An Equal Opportunity Employer Open Competitive Examination Exam Title: Director of Public Works (Town of Rotterdam) Town of Rotterdam The resulting eligible list will be used to fill
Schenectady County Is An Equal Opportunity Employer Open Competitive Examination Exam Title: Director of Public Works (Town of Rotterdam) Town of Rotterdam The resulting eligible list will be used to fill
Advertisement No. 2/2013
 OFFICE OF THE REGISTRAR ASSAM AGRICULTURAL UNIVERSITY JORHAT-785013 Advertisement No. 2/2013 Applications from the Indian citizens are invited for 19 (nineteen) posts of Jr. Scientists and equivalent rank
OFFICE OF THE REGISTRAR ASSAM AGRICULTURAL UNIVERSITY JORHAT-785013 Advertisement No. 2/2013 Applications from the Indian citizens are invited for 19 (nineteen) posts of Jr. Scientists and equivalent rank
Certification Requirements
 Certification Requirements Office of Education North American Division of Seventh day Adventists 2002 All requirements within this document are mandatory for certification or recertification beginning
Certification Requirements Office of Education North American Division of Seventh day Adventists 2002 All requirements within this document are mandatory for certification or recertification beginning
AMERICAN OSTEOPATHIC BOARD OF PREVENTIVE MEDICINE
 AMERICAN OSTEOPATHIC BOARD OF PREVENTIVE MEDICINE 2017 APPLICATION HANDBOOK Primary Certifications Aerospace Medicine Occupational/Environmental Medicine Public Health/Community Medicine Certificate of
AMERICAN OSTEOPATHIC BOARD OF PREVENTIVE MEDICINE 2017 APPLICATION HANDBOOK Primary Certifications Aerospace Medicine Occupational/Environmental Medicine Public Health/Community Medicine Certificate of
Admission ADMISSIONS POLICIES APPLYING TO BISHOP S UNIVERSITY. Application Procedure. Application Deadlines. CEGEP Applicants
 Admission General inquiries from prospective students should be directed to: Recruitment Office Bishop s University 2600 College Street Sherbrooke, Quebec J1M 1Z7 Tel. 819-822-9600 ext. 2681 or 1 877-822-8200
Admission General inquiries from prospective students should be directed to: Recruitment Office Bishop s University 2600 College Street Sherbrooke, Quebec J1M 1Z7 Tel. 819-822-9600 ext. 2681 or 1 877-822-8200
SAMPLE AFFILIATION AGREEMENT
 SAMPLE AFFILIATION AGREEMENT AFFILIATION AGREEMENT FOR USE WITH A FOREIGN STUDY PROGRAM W I T N E S S E T H and WHEREAS, cordial relations exist between the United Stated of America and France; WHEREAS,
SAMPLE AFFILIATION AGREEMENT AFFILIATION AGREEMENT FOR USE WITH A FOREIGN STUDY PROGRAM W I T N E S S E T H and WHEREAS, cordial relations exist between the United Stated of America and France; WHEREAS,
College of Engineering and Applied Science Department of Computer Science
 College of Engineering and Applied Science Department of Computer Science Guidelines for Doctor of Philosophy in Engineering Focus Area: Security Last Updated April 2017 I. INTRODUCTION The College of
College of Engineering and Applied Science Department of Computer Science Guidelines for Doctor of Philosophy in Engineering Focus Area: Security Last Updated April 2017 I. INTRODUCTION The College of
Placentia-Yorba Linda Unified School District 1301 E. Orangethorpe Ave., Placentia, CA (714)
") 1 INTERNATIONAL STUDENTS Welcome to the. This information is for international students who are seeking a one year public high school experience for Grades 9-12. Esperanza High School (www.esperanzahs.net),
1 INTERNATIONAL STUDENTS Welcome to the. This information is for international students who are seeking a one year public high school experience for Grades 9-12. Esperanza High School (www.esperanzahs.net),
ARLINGTON PUBLIC SCHOOLS Discipline
 All staff members of the Arlington Public Schools have authority to maintain the orderly behavior of students. Students in Arlington Public Schools are expected to demonstrate responsibility and self-discipline
All staff members of the Arlington Public Schools have authority to maintain the orderly behavior of students. Students in Arlington Public Schools are expected to demonstrate responsibility and self-discipline
Sl. No. Name of the Post Pay Band & Grade Pay No. of Post(s) Category
 Category") National Institute of Open Schooling (An autonomous organization under the Deptt. of School Education & Literacy, MHRD Govt. of India) A-24-25, Institutional Area, Sector 62, NOIDA- 201309, Uttar Pradesh
National Institute of Open Schooling (An autonomous organization under the Deptt. of School Education & Literacy, MHRD Govt. of India) A-24-25, Institutional Area, Sector 62, NOIDA- 201309, Uttar Pradesh
Spring 2015 CRN: Department: English CONTACT INFORMATION: REQUIRED TEXT:
 Harrisburg Area Community College Virtual Learning English 104 Reporting and Technical Writing 3 credits Spring 2015 CRN: 32330 Department: English Instructor: Professor L.P. Barnett Office Location: York
Harrisburg Area Community College Virtual Learning English 104 Reporting and Technical Writing 3 credits Spring 2015 CRN: 32330 Department: English Instructor: Professor L.P. Barnett Office Location: York
West Hall Security Desk Attendant Application
 West Hall Security Desk Attendant Application Mail Completed Application To: Office of Residence Life Attn: SDA Application 100 State Street, PO Box 9101 Framingham, MA 01701-9101 OR Drop Off Completed
West Hall Security Desk Attendant Application Mail Completed Application To: Office of Residence Life Attn: SDA Application 100 State Street, PO Box 9101 Framingham, MA 01701-9101 OR Drop Off Completed
Oklahoma State University Policy and Procedures
 Oklahoma State University Policy and Procedures REAPPOINTMENT, PROMOTION AND TENURE PROCESS FOR RANKED FACULTY 2-0902 ACADEMIC AFFAIRS September 2015 PURPOSE The purpose of this policy and procedures letter
Oklahoma State University Policy and Procedures REAPPOINTMENT, PROMOTION AND TENURE PROCESS FOR RANKED FACULTY 2-0902 ACADEMIC AFFAIRS September 2015 PURPOSE The purpose of this policy and procedures letter
Article 15 TENURE. A. Definition
 Article 15 TENURE A. Definition Tenure shall mean the right of a FACULTY MEMBER to hold his/her position and not to be removed therefrom except for just cause as hereinafter set forth in this Article or
Article 15 TENURE A. Definition Tenure shall mean the right of a FACULTY MEMBER to hold his/her position and not to be removed therefrom except for just cause as hereinafter set forth in this Article or
Oakland University OU STEP
 Application to Program This packet includes the information, instructions, and forms that you will need to submit an application to the Oakland University Secondary Teacher Education Program (). The STEP
Application to Program This packet includes the information, instructions, and forms that you will need to submit an application to the Oakland University Secondary Teacher Education Program (). The STEP
Application for Fellowship Leave
 PDF Fill-In Form: Type On-Screen, then Print for Signatures and Chair Approvals Brooklyn College (2018-2019 Academic Year) Application for Fellowship Leave Instructions for Applicant: Please complete Sections
PDF Fill-In Form: Type On-Screen, then Print for Signatures and Chair Approvals Brooklyn College (2018-2019 Academic Year) Application for Fellowship Leave Instructions for Applicant: Please complete Sections
Surgical Residency Program & Director KEN N KUO MD, FACS
 Surgical Residency Program & Director KEN N KUO MD, FACS 1 Taiwan Surgical Association Residency Director Meeting September 17, 2011 November 5, 2011 2 Three Stages of Education Undergraduate medical education
Surgical Residency Program & Director KEN N KUO MD, FACS 1 Taiwan Surgical Association Residency Director Meeting September 17, 2011 November 5, 2011 2 Three Stages of Education Undergraduate medical education
GRADUATE SCHOOL DOCTORAL DISSERTATION AWARD APPLICATION FORM
 READ THESE INSTRUCTIONS BEFORE FILLING IN THE APPLICATION Purpose The University of Florida (UF) Graduate School Doctoral Dissertation Award is a competitive, need based award program to provide final
READ THESE INSTRUCTIONS BEFORE FILLING IN THE APPLICATION Purpose The University of Florida (UF) Graduate School Doctoral Dissertation Award is a competitive, need based award program to provide final
Southeast Arkansas College 1900 Hazel Street Pine Bluff, Arkansas (870) Version 1.3.0, 28 July 2015
 Version 1.3.0, 28 July 2015") Southeast Arkansas College 1900 Hazel Street Pine Bluff, Arkansas 71603 www.seark.edu (870) 543-5900 Version 1.3.0, 28 July 2015 Concurrent Credit Student Handbook 2015/16 Table of Contents What is Concurrent
Southeast Arkansas College 1900 Hazel Street Pine Bluff, Arkansas 71603 www.seark.edu (870) 543-5900 Version 1.3.0, 28 July 2015 Concurrent Credit Student Handbook 2015/16 Table of Contents What is Concurrent
Cy-Fair College Teacher Preparation and Certification Program Application Form
 Cy-Fair College Teacher Preparation and Certification Program Application Form Date Name (circle one) Mr. Mrs. Ms. Miss. (Last, First, Middle) Address (Number, Street, Apartment Number) (City, State, Zip)
Cy-Fair College Teacher Preparation and Certification Program Application Form Date Name (circle one) Mr. Mrs. Ms. Miss. (Last, First, Middle) Address (Number, Street, Apartment Number) (City, State, Zip)
Kelso School District and Kelso Education Association Teacher Evaluation Process (TPEP)
") Kelso School District and Kelso Education Association 2015-2017 Teacher Evaluation Process (TPEP) Kelso School District and Kelso Education Association 2015-2017 Teacher Evaluation Process (TPEP) TABLE
Kelso School District and Kelso Education Association 2015-2017 Teacher Evaluation Process (TPEP) Kelso School District and Kelso Education Association 2015-2017 Teacher Evaluation Process (TPEP) TABLE
HIGHLAND HIGH SCHOOL CREDIT FLEXIBILITY PLAN
 HIGHLAND HIGH SCHOOL CREDIT FLEXIBILITY PLAN TABLE OF CONTENTS Overview 1 Eligible Credit Flexibility Plans 2 Earned Credit from Credit Flexibility Plans 2 Student Athletes 3 Application Process 3 Final
HIGHLAND HIGH SCHOOL CREDIT FLEXIBILITY PLAN TABLE OF CONTENTS Overview 1 Eligible Credit Flexibility Plans 2 Earned Credit from Credit Flexibility Plans 2 Student Athletes 3 Application Process 3 Final
Anyone with questions is encouraged to contact Athletic Director, Bill Cairns; Phone him at or
 SKYLINE GRIZZLIES ATHLETIC REQUIREMENTS and REGISTRATION FORMS 2017-18 According to School District #91 and Idaho High School Activities Association rules, all students interested in participating in athletics
SKYLINE GRIZZLIES ATHLETIC REQUIREMENTS and REGISTRATION FORMS 2017-18 According to School District #91 and Idaho High School Activities Association rules, all students interested in participating in athletics
Vocational Training. Pre-Application
 Vocational Training Pre-Application 1 Vocational Training Application Checklist Dear Prospective Student: Congratulation on your choice to continue your education at an institute of Higher learning! Unfortunately,
Vocational Training Pre-Application 1 Vocational Training Application Checklist Dear Prospective Student: Congratulation on your choice to continue your education at an institute of Higher learning! Unfortunately,
Northern Virginia Alumnae Chapter of Delta Sigma Theta Sorority, Incorporated Scholarship Application Guidelines and Requirements
 P.O. Box 4310 Arlington, VA 22204 9998 novac@dstnovac.org Northern Virginia Alumnae Chapter of Delta Sigma Theta Sorority, Incorporated Scholarship Application Guidelines and Requirements In 2017, the
P.O. Box 4310 Arlington, VA 22204 9998 novac@dstnovac.org Northern Virginia Alumnae Chapter of Delta Sigma Theta Sorority, Incorporated Scholarship Application Guidelines and Requirements In 2017, the
14820 Serenita Avenue Oklahoma City, OK COURSE CATALOG
 14820 Serenita Avenue Oklahoma City, OK 73134 405.609.6622 WWW.CENTRALOC.EDU COURSE CATALOG Catalog Effective April 10, 2017 1 TABLE OF CONTENTS ABOUT US 3 HISTORY 3 MISSION STATEMENT 3 APPROVALS AND LICENSES
14820 Serenita Avenue Oklahoma City, OK 73134 405.609.6622 WWW.CENTRALOC.EDU COURSE CATALOG Catalog Effective April 10, 2017 1 TABLE OF CONTENTS ABOUT US 3 HISTORY 3 MISSION STATEMENT 3 APPROVALS AND LICENSES
Youth Apprenticeship Application Packet Checklist
 Youth Apprenticeship Application Packet Checklist Incomplete applications will not be forwarded to hiring companies and will delay the application process. A complete application packet should consist
Youth Apprenticeship Application Packet Checklist Incomplete applications will not be forwarded to hiring companies and will delay the application process. A complete application packet should consist
Meeting these requirements does not guarantee admission to the program.
 .Eastern Connecticut State University, School of Education & Professional Studies Committee on Admission and Retention in Education (CARE) UNDERGRADUATE ELEMENTARY Teacher Certification Application Application
.Eastern Connecticut State University, School of Education & Professional Studies Committee on Admission and Retention in Education (CARE) UNDERGRADUATE ELEMENTARY Teacher Certification Application Application
ARTICLE IV: STUDENT ACTIVITIES
 ARTICLE IV: STUDENT ACTIVITIES Table of Contents 7-4.1 extracurricular Activities: Generally 7-4.2 sportsmanship, ethics and integrity 7-4.3 student publications 7-4.4 assemblies 7-4.5 clubs and student
ARTICLE IV: STUDENT ACTIVITIES Table of Contents 7-4.1 extracurricular Activities: Generally 7-4.2 sportsmanship, ethics and integrity 7-4.3 student publications 7-4.4 assemblies 7-4.5 clubs and student
Frequently Asked Questions and Answers
 Definition and Responsibilities 1. What is home education? Frequently Asked Questions and Answers Section 1002.01, F.S., defines home education as the sequentially progressive instruction of a student
Definition and Responsibilities 1. What is home education? Frequently Asked Questions and Answers Section 1002.01, F.S., defines home education as the sequentially progressive instruction of a student
DEPARTMENT OF EXAMINATIONS, SRI LANKA GENERAL CERTIFICATE OF EDUCATION (ADVANCED LEVEL) EXAMINATION - AUGUST 2016
 EXAMINATION - AUGUST 2016") DEPARTMENT OF EXAMINATIONS, SRI LANKA GENERAL CERTIFICATE OF EDUCATION (ADVANCED LEVEL) EXAMINATION - AUGUST 2016 Applications of private candidates for the above examination will be received from 01.02.2016
DEPARTMENT OF EXAMINATIONS, SRI LANKA GENERAL CERTIFICATE OF EDUCATION (ADVANCED LEVEL) EXAMINATION - AUGUST 2016 Applications of private candidates for the above examination will be received from 01.02.2016
Academic Freedom Intellectual Property Academic Integrity
 Academic Policies The purpose of Gwinnett Tech s academic policies is to ensure fairness and consistency in the manner in which academic performance is administered, evaluated and communicated to students.
Academic Policies The purpose of Gwinnett Tech s academic policies is to ensure fairness and consistency in the manner in which academic performance is administered, evaluated and communicated to students.
I. General provisions. II. Rules for the distribution of funds of the Financial Aid Fund for students
 Rules and Regulations for the calculation, awarding and payment of financial aid for full-time and part-time students with awarding criteria and procedures at the Warsaw Film School I. General provisions
Rules and Regulations for the calculation, awarding and payment of financial aid for full-time and part-time students with awarding criteria and procedures at the Warsaw Film School I. General provisions
Schock Financial Aid Office 030 Kershner Student Service Center Phone: (610) University Avenue Fax: (610)
 University Avenue Fax: (610)") Schock Financial Aid Office 030 Kershner Student Service Center Phone: (610) 436-2627 25 University Avenue Fax: (610) 436-2574 West Chester, PA 19383 E-Mail: finaid@wcupa.edu Title IV Federal Student Aid
Schock Financial Aid Office 030 Kershner Student Service Center Phone: (610) 436-2627 25 University Avenue Fax: (610) 436-2574 West Chester, PA 19383 E-Mail: finaid@wcupa.edu Title IV Federal Student Aid
Application Paralegal Training Program. Important Dates: Summer 2016 Westwood. ABA Approved. Established in 1972
 Business, Management & Legal Programs Application 2016-2017 Important Dates: Summer 2016 Westwood Paralegal Training Program Monday to Friday, 9am to 12:30pm Application Deadline: May 27, 2016* Program
Business, Management & Legal Programs Application 2016-2017 Important Dates: Summer 2016 Westwood Paralegal Training Program Monday to Friday, 9am to 12:30pm Application Deadline: May 27, 2016* Program
Bachelor of International Hospitality Management, BA IHM. Course curriculum National and Institutional Part
 Bachelor of International Hospitality Management, BA IHM Course curriculum 2016-2018 August 2016 0 INDHOLD 1. curriculum framework... 4 1.1. Objective of the study programme... 4 1.2. Title and duration...
Bachelor of International Hospitality Management, BA IHM Course curriculum 2016-2018 August 2016 0 INDHOLD 1. curriculum framework... 4 1.1. Objective of the study programme... 4 1.2. Title and duration...
Spring Valley Academy Credit Flexibility Plan (CFP) Overview
 Overview") Overview Ohio Senate Bill 311 allows alternate pathways for those students who are eligible to receive high school credit through the use of Credit Flexibility Plans (CFPs). Spring Valley Academy students
Overview Ohio Senate Bill 311 allows alternate pathways for those students who are eligible to receive high school credit through the use of Credit Flexibility Plans (CFPs). Spring Valley Academy students
Proposed Amendment to Rules 17 and 22 of the Rules of the Supreme Court of the State of Hawai i MANDATORY CONTINUING LEGAL EDUCATION
 RE: Proposed Amendment to Rules 17 and 22 of the Rules of the Supreme Court of the State of Hawai i MANDATORY CONTINUING LEGAL EDUCATION The Supreme Court of Hawai i seeks public comment regarding proposals
RE: Proposed Amendment to Rules 17 and 22 of the Rules of the Supreme Court of the State of Hawai i MANDATORY CONTINUING LEGAL EDUCATION The Supreme Court of Hawai i seeks public comment regarding proposals
Perioperative Care of Congenital Heart Diseases
 CALL FOR APPLICATIONS DR 617/2017 II LEVEL MASTER Perioperative Care of Congenital Heart Diseases Academic Year 2017/2018 2018/2019 In collaboration with Fondazione G. Monasterio Regione Toscana CNR Article
CALL FOR APPLICATIONS DR 617/2017 II LEVEL MASTER Perioperative Care of Congenital Heart Diseases Academic Year 2017/2018 2018/2019 In collaboration with Fondazione G. Monasterio Regione Toscana CNR Article
Living on Campus. Housing and Food Services
 Living on Campus at At the the center Center of of it It all. All 1406 Asp Ave., Room 126 Norman, OK 73019 Phone: 405-325-1284 FAX: 405-325-7117 1406 Asp Ave., Room 126 E-Mail: info@housing.ou.edu Norman,
Living on Campus at At the the center Center of of it It all. All 1406 Asp Ave., Room 126 Norman, OK 73019 Phone: 405-325-1284 FAX: 405-325-7117 1406 Asp Ave., Room 126 E-Mail: info@housing.ou.edu Norman,